- Research article
- Open access
- Published:
Proposal for a classification system of radiographic bone changes after cervical disc replacement
Journal of Orthopaedic Surgery and Research volume 19, Article number: 218 (2024)
Abstract
Background
The goal of this study is to propose a classification system with a common nomenclature for radiographic observations of periprosthetic bone changes following cTDR.
Methods
Aided by serial plain radiographs from recent cTDR cases (34 patients; 44 devices), a panel of experts assembled for the purpose of creating a classification system to aid in reproducibly and accurately identifying bony changes and assessing cTDR radiographic appearance. Subdividing the superior and inferior vertebral bodies into 3 equal sections, observed bone loss such as endplate rounding, cystic erosion adjacent to the endplate, and cystic erosion not adjacent to the endplate, is recorded. Determining if bone loss is progressive, based on serial radiographs, and estimating severity of bone loss (measured by the percentage of end plate involved) is recorded. Additional relevant bony changes and device observations include radiolucent lines, heterotopic ossification, vertebral body olisthesis, loss of core implant height, and presence of device migration, and subsidence.
Results
Serial radiographs from 19 patients (25 devices) implanted with a variety of cTDR designs were assessed by 6 investigators including clinicians and scientists experienced in cTDR or appendicular skeleton joint replacement. The overall agreement of assessments ranged from 49.9% (95% bootstrap confidence interval 45.1–73.1%) to 94.7% (95% CI 86.9–100.0%). There was reasonable agreement on the presence or absence of bone loss or radiolucencies (range: 58.4% (95% CI 51.5–82.7%) to 94.7% (95% CI 86.9–100.0%), as well as in the progression of radiolucent lines (82.9% (95% CI 74.4–96.5%)).
Conclusions
The novel classification system proposed demonstrated good concordance among experienced investigators in this field and represents a useful advancement for improving reporting in cTDR studies.
Introduction
Cervical total disc replacement (cTDR) is becoming an established alternative to fusion for treatment of degenerative disc disease and associated radiculopathy and myelopathy [1,2,3,4]. Starting in the 2000s, the clinical effectiveness of cTDR has been supported by randomized clinical trials, now with intermediate- and long-term follow-up [2, 4,5,6,7,8,9,10]. Early cTDR designs were often based on traditional orthopaedic biomaterials, including polyethylene, CoCr alloys and Ti alloys [3, 10], but the lower biomechanical loading demands of the cervical spine relative to the lumbar spine have also encouraged innovative designers to investigate new bearing materials [11], incorporating metallic alloys, ceramics, polycarbonate urethane, and/or PEEK, with no previous clinical precedent as bearing materials in large total joint replacements. As cTDR designs and its biomaterials continue to evolve, and as utilization of the procedure increases with longer historical exposure, there has been increased attention on identifying mechanisms of cTDR failure [12], such as subsidence, migration, and/or wear, along with recommended treatment paradigms for each clinical failure scenario [12]. Ideally, classification and treatment pathways should be generalized with the understanding that cTDR failures, and their revision approaches, may be design specific.
Since the beginning of large-joint arthroplasty, clinicians and orthopedic researchers have used radiographs to evaluate the status of implant fixation and the likelihood of impending revision surgery. For example, Delee and Charnley [13] and Gruen [14] proposed acetabular and femoral zones in the 1970s which later came to be widely used in describing the location and progression of radiolucent lines and osteolytic lesions around a total hip replacement. Progressive radiolucent lines around a hip component of greater than 2 mm have been found to be associated with clinically relevant loosening that may require revision [13, 15]. However, an equivalent, generally accepted radiographic classification and treatment approach is not yet available in cTDR, in part because of the recent adoption of this relatively new procedure, and also because of the diversity in implant designs. The clinical situation is more complex in cTDR than in large joints, in which diagnosis and treatment are generally based on radiographic examination as the “keystone” diagnostic tool [15]. By contrast, cTDR treatment decisions involving revision are less frequently undertaken based on radiographs alone, without further workup that may include computed tomography (CT) scans and/or magnetic resonance imaging (MRI). Of these imaging modalities, CT is the most reliable test for bone loss.
Nevertheless, plain radiographic assessment remains the front-line patient assessment tool for cTDR [12, 16]. Previous studies have underscored the need for classification of radiographic changes around cTDR including heterotopic ossification (HO) [17, 18] and bone loss [12, 19]. Bone loss around orthopedic implants can result from sepsis [20, 21], or aseptically due to bone adaptation or remodeling due to stress shielding (sometimes referred to as “Wolff’s law”) [22], osteoporosis [23], fluid pressure [24], as well as the well-described chronic inflammatory reaction to wear debris termed “osteolysis” in peripheral joint arthroplasty [19]. Today, the etiology of bone loss around large-joint implants can be effectively elucidated with plain radiographs and long-term clinical experience with specific designs [15], but whether a radiographic bone lesion is septic or aseptic, or due to bone adaptation or particulate wear debris, may require confirmation by pathologic examination of retrieved periprosthetic tissues [25] as well as microbiological cultures of synovial fluid and periprosthetic tissues.
However, authors in the spine field often use terms such as wear, osteolysis, and bone loss interchangeably to describe radiographic changes around cTDRs, without pathologic confirmation for the etiology of bone loss [19, 26, 27]. Zavras et al. [12] have recently proposed a cTDR failure classification system, with wear as a type of failure with subclassification of osteolysis with minimal or severe bone loss. The ambiguity and lack of specificity in the radiographic assessment of periprosthetic bony changes around cTDR is a barrier to effective scientific communication and the development of effective treatment recommendations.
Consequently, the purpose of the present study was to develop and assess a radiographic classification system for reactive changes after cTDR. We sought to answer the following principal research question: can plain radiographs be used for accurate and repeatable classification of bony changes after cTDR? To answer this question, our team developed and evaluated a classification system using blinded and de-identified radiographic case studies drawn from their clinical experience with multiple implant designs.
Methods
Development of the classification system
A classification system in the present study was iteratively developed over a 12-month period, during which the co-authors convened as a panel to collaboratively evaluate serial radiographs of cTDRs and previous classification studies for cTDR [12, 18, 19, 28] and total joint replacement [13, 14]. The panel consisted of six investigators, including four experienced cTDR surgeons (AK, FP, TL, GA), an experienced large joint orthopaedic surgeon (JJ), and a clinical researcher (SMK) with experience in TDR revision and assessment of bony changes in radiographs around large total joint replacements. Because our goal was to assess radiographic changes over time, and cTDRs routinely exhibit gaps or radiolucent lines immediately after implantation that gradually fill in over time, assessments were not made based on an isolated set of radiographs. This approach was consistent with best practices of assessing bony changes around hip and knee total joints. We initially considered the use of anterior–posterior (AP) radiographs as part of the classification system, however we found that the APs of the cTDR cases available to us were more variable in terms of readability and angle of the incident beam, making evaluation of the interface more difficult. Hence, we relied on lateral radiographs as the basis for our classification system. Radiographs from 34 patients representing 44 implants from 7 implant systems were reviewed to aid in the development of the classification system, specifically for the purpose of identifying and agreeing on bone change descriptions and important implant considerations. The radiographs were sourced from the spine surgeon coauthors’ recent cTDR cases, in particular those with exemplary imaging.
The classification protocol for assessing radiographic changes was based on lateral plain radiographs of the cervical spine, dividing the vertebral body into three sections, anterior, middle, posterior, approximating sections as shown in Fig. 1. Attention was focused on characterizing changes around both the superior and inferior endplates in these three sections. Note that these figures are artists renderings of radiographs to convey the particular observed anatomy. Example of radiographs from patients used in the study are included in the Additional file 1.

Schematic of six periprosthetic regions for assessment of bony changes after cTDR based on lateral radiographs: superior posterior (SP), superior middle (SM), superior anterior (SA), inferior posterior (IP), inferior middle (IM), inferior anterior (IA)
Bony changes of potential clinical relevance may include:
-
1.
Endplate Rounding (Fig. 2a). This type of bony change has previously been observed around many types of implant designs [28, 29].
-
2.
Cystic Erosion Adjacent to Endplate w/ Diffuse Margin. This type of change can manifest as a radiolucent shadow with poorly defined border (Fig. 2b).
-
3.
Cystic Erosion Adjacent to Endplate w/ Sclerotic Margin. This manifests as a radiolucent shadow with defined border of radiodense bone (Fig. 2c).
-
4.
Cystic Bone Loss Not Adjacent to the Endplate (Fig. 2d).

Bony changes of potential clinical relevance around cTDR: A Endplate Rounding; B Cystic Erosion Adjacent to Endplate w/Diffuse Margin; C Cystic Erosion Adjacent to Endplate w/Sclerotic Margin; D Cystic Bone Loss Not Adjacent to the Endplate
The severity of the bone loss (i.e., the degree to which the endplates are unsupported) was assessed using the following characterization scheme:
-
1.
None = Neither endplate exhibits bone loss
-
2.
Mild = If either endplate exhibits bone loss that includes an unsupported portion of the endplate that is less than 1/6th of the endplate
-
3.
Moderate = If either endplate exhibits bone loss that includes an unsupported portion of the endplate that is between 1/6th and 1/3rd of the endplate
-
4.
Severe = If either endplate exhibits bone loss that includes an unsupported portion of the endplate that is more than 1/3rd of the endplate
Note that these changes were recorded only if they were not apparent on the immediate postoperative X-rays. Serial radiographs were required to judge the presence and severity of progression. Progression was recorded if the severity of the bony changes (as defined above) increased between the two most recent follow up radiographic series. If there is only one follow up radiographic series after the immediate postoperative films, the determination of progression is far less meaningful; it has been our observation that bony changes up to two years postoperatively may stabilize, showing no further progression on further follow up, up to 5 years.
We also developed a classification scheme to identify the location of radiolucent lines and noted if they were progressive. In the hip and knee literature, radiolucent lines of greater than 2 mm are generally considered to be indicative of implant loosening, however utility of assessing radiolucent lines at the bone implant interface of cTDR is less well defined. Therefore, based on the cTDR images in the present study, we identified the presence of radiolucent lines at the bone implant interface, regardless of their thickness.
Heterotopic ossification (HO) is frequently observed after cTDR and therefore included in the present study. In each of the assessment regions, we identified HO formation on the most recent radiograph based on McAfee classification system [18]:
-
1.
Class 0—No HO present
-
2.
Class I—Presence of HO in front of vertebral body but not in the anatomic disc space
-
3.
Class II—Presence of HO in the disc space, possible affecting the prosthesis’s function.
-
4.
Class III—Bridging HO with prosthesis’s motion still preserved.
-
5.
Class IV—Complete fusion of the segment with absence of motion in flexion/extension.
We also characterized the changes to the implant and its intervertebral positioning. Core implant height is commonly used to assess the performance of the implant over its lifetime by comparing serial radiographs over time, looking for changes in the height of the implant. Core implant height changes were classified as either none/minor (< 50% height loss) or moderate/collapse (> 50% height loss). Similarly, migration, subsidence, and distortion of the core with olisthesis were noted (yes/no). Migration and subsidence can be difficult to quantify. Some hip replacement studies have used 3 mm as a threshold [30], but in cervical application, this is less defined. Therefore, these were noted as either present or not (yes/no), based on the available information of the case. Migration was defined as anterior/posterior/medial/lateral movement of implant relative to vertebral body as compared between immediate post-op and most current radiograph. Subsidence was defined as superior/inferior movement of implant relative to vertebral body as compared between immediate post-op and most current radiograph. Olisthesis was used to describe translation of superior endplate of well-fixed implants relative to the inferior endplate. Spondylolisthesis was used to describe translation of the superior endplate anterior with respect to the inferior endplate. Retrolisthesis was used to describe translation of the superior endplate posterior with respect to the inferior endplate. As with all radiographic assessment and to use the proposed classification system effectively, the importance of good quality, well positioned, serial radiographs for assessment is very important, as this can affect the ability to assess the bony changes.
In developing the classification system, several iterations of general protocol and data collection form were generated. Figures 3 and 4 detail the protocol provided to the investigators as well as the form used to collect their observations.
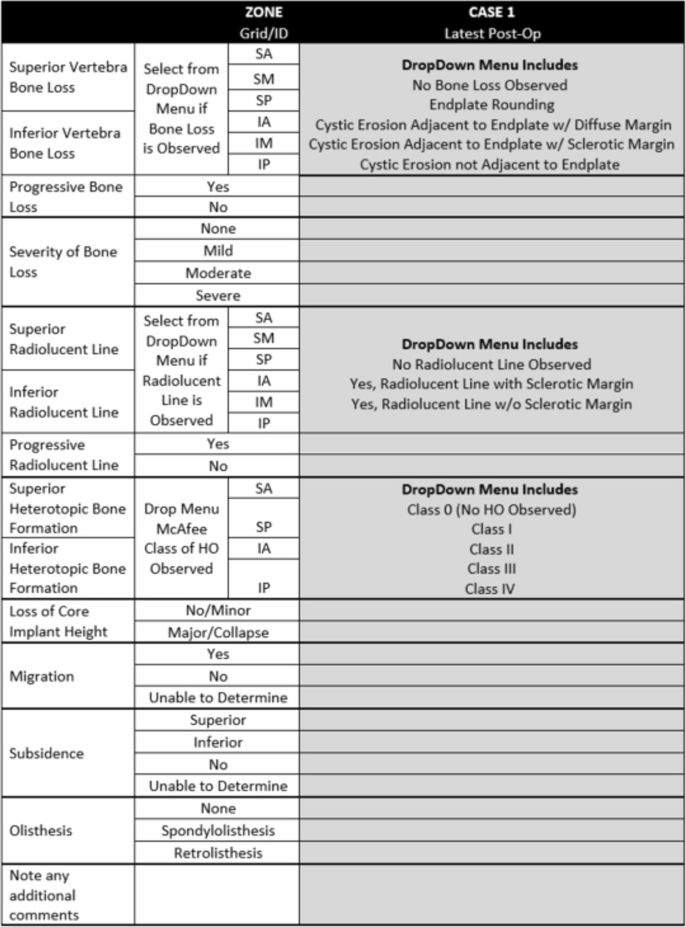
Case report form used to collect data

Protocol used for assessment of bone loss from radiographs
Gathering the data
The case series for the present study was an assembly of serial radiographs from cTDR cases by the spine surgeon investigators. The study protocol was reviewed by an external IRB and found to be IRB exempt.
For the present study, the serial radiographs from 19 patients with 25 implants were assembled and assessed using the classification system. The case series was assembled based on historical cases from the 4 spine surgeon investigators, and because radiographic changes were the focus of the assessment, inclusion of cases was based on availability of serial radiographs. For a case to be included, radiographs from pre-operative, post-operative, and latest follow-up timepoints had to be available, along with clinical presentation information. The pre-operative radiograph was crucial for understanding existing bone condition/anomalies prior to implant-related bone changes, and utilizing cases from a variety of manufacturers and designs helped reduce bias and focus on bone changes. Specific implantation duration was not required. The cases included the following implant systems: Discover (n = 1 patient, DePuy Spine), ProDisc-C (n = 2; Centinel Spine), Simplify (n = 2; NuVasive), M6-C (n = 5; Orthofix), Prestige LP (n = 2; Medtronic), Mobi-C (n = 9; ZimVie), and PCM (n = 4, NuVasive). There were 14 single-level patients, 4 two-level patients, and 1 three-level patient included as part of the study.
To simulate clinical situation as closely as possible, in evaluating case series, panel members considered patient reported symptoms throughout the course of their treatment and serial radiographs typically including index surgery, one-, two-, and five-years post-op. The 6 investigators were provided de-identified serial radiographs and clinical information for each case in the series. The clinical symptoms were used by the investigators to consider potential issues that might be observed in the radiographs, such as common bone loss scenarios, implant performance, potential bony abnormalities, or unique radiographic findings. This information was captured in the notes section of the data collection form (Fig. 4). Independently, each investigator reviewed each case according to the protocol, and provided observations using the data collection form. The data was then pooled, and statistical analyses conducted.
Statistical methods
The concordance between investigators was found by multiple pairwise comparison of investigator assessments. The maximum number of pairwise comparisons was 375. Concordance was determined by the number of paired observations, as compared with the total number of possible paired comparisons among investigators. Thus, if all of the paired comparisons in each of the region were consistent, that would result in 100% concordance or agreement (375 matching assessments out of a maximum 375 total possible assessments).
A random effects model was hypothesized as the data generating mechanism in order to evaluate the uncertainty in the estimates of overall agreement for each measurement. The model assumed that the 6 raters and 25 subjects were selected at random from populations of raters and subjects. A bootstrapping approach [31] was used to determine empirical sampling distributions for overall agreement. This was accomplished by creating 500 bootstrap samples by sampling 6 raters from the set of available raters with replacement and sampling 25 subjects from the set of available subjects with replacement; and then determining overall agreement as usual for each sample. The lower and upper bounds of the 95% confidence intervals were determined non-parametrically as the 2.5th and 97.5th percentile values. Agreement values smaller than lower bounds of the confidence intervals may be statistically ruled out. Overall agreement may be more interpretable in many cases than Kappa or Krippendorff’s Alpha values, which are very similar, are chance adjusted agreement rates but depend highly on prevalence of individual findings and marginal distributions (Fig. 5).
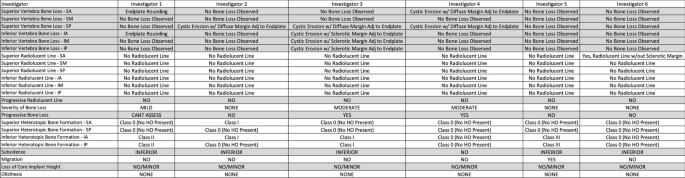
Example of case assessment data from six investigators
Results
The overall agreement of assessments ranged from 49.9% (45.1–73.1%) to 94.7% (86.9–100.0%) (Table 1). There was reasonable agreement on the presence or absence of bone loss or radiolucencies (range: 58.4 (51.5–82.7%) to 94.7% (86.9–100.0%), Table 1), as well as in the progression of radiolucent lines (82.9% (74.4–96.5%)). However, the lowest agreement was found on the assessment of severity of bone loss (49.9% (45.1–73.1%)) or the progression of bone loss (66.2% (59.7–87.7%)). High overall agreement was achieved in binary assessments of HO (range: 75.2 (66.9–91.5%) to 91.7% (83.2–100.0%)) and implant function, such as the presence of subsidence (82.2% (73.1–94.9%)), migration (90.3% (83.2–100.0%)), loss of core implant height (90.9% (83.2–100.0%)), and olisthesis (72.0% (64.8–91.7%)).
Discussion
As the usage of cervical arthroplasty has increased over the past 20 years, the prevalence of clinical and device-related failures associated with this technology has also increased, motivating the present study to develop a clinically useful classification system to aide clinicians with assessing bony changes over time. In the present study, we developed a robust classification scheme for bony changes around cTDR that was evaluated across a broad range of contemporary implant designs. We utilized serial radiographs of routine clinical cases in our radiographic assessment of cTDR. It became increasingly clear during our collaboration how important serial radiographs are in accurately assessing any progression of bone loss. We routinely found evidence of bone-implant gaps upon assessment of post-operative radiographs that did not fill in or remodel up to five years of implantation. Without access to serial radiographs, those initial unresolved bone-implant gaps could be misinterpreted as bone loss. Therefore, if only a single radiographic observation is available, clinical interpretation is problematic, and additional imaging studies, including computed tomography (CT) and magnetic resonance imaging (MRI) are strongly recommended prior to undertaking further clinical intervention.
There are relatively few studies that have addressed classification of cTDR failure modes that focus specifically on the bone-implant interface [12]. Zavras et al. [12] proposed a general classification for cTDR reasons for revision, that specifically focused on failures that required revision surgery. Zavras and colleagues also classified revision due to septic loosening as a sub classification of infection, whereas revisions due to implant wear were subclassified as either with or without osteolysis. The implication of Zavras’ classification system is that osteolysis is solely associated with wear-related failure of cTDR. We certainly agree with Zavras’ identification of wear as a potential mechanism for osteolysis in the spine, however given that other mechanisms can result in periprosthetic bone loss, such as infection and stress-shielding, we underscore the importance of classifying bone loss based on imaging without attribution of etiology until histopathological confirmation of the root cause has been determined [19]. In large joint orthopaedics, decades of early fixation methods and historical polyethylene bearing materials resulted in radiographic classification systems for bone loss that reflected a time when particulate wear debris from bone cement, metal, and polyethylene was responsible for many more clinical failures than infection. A similar situation does not occur today with cTDR, in which wear related revisions and infection as documented in prospective randomized clinical trials [2, 5,6,7,8,9], are both equally low in incidence, and hence the etiology of periprosthetic bone loss associated with cTDR cannot be reliably assumed based on radiographs alone. In hip and knee replacements, clinical experience has evolved over decades to educate the intuition of surgeons with the radiographic interpretation of bone loss due to non-inflammatory bone adaptation in comparison with inflammatory mechanisms of osteolysis such as infection and particulate wear debris [19]. However, this is not the case with cTDR in which the clinical experience with radiographic interpretation of periprosthetic bony changes is still relatively early in its development. Although osteolysis around cTDR has been raised as a potential clinical concern [19, 27], the use of a reliable radiographic classification system as proposed here, coupled with device and tissue retrieval analysis, should improve future scientific communications about bone loss around total disc replacements, along with their reasons for revision.
Radiographic outcomes are publicly reported for cTDR designs that have completed clinical trials as part of their regulatory approval process by the United States Food and Drug Administration (FDA) (https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm). Radiographic outcomes and observations were extracted from the summaries of safety and effectiveness (SSED) from 12 FDA-approved cTDRs currently on the US market and summarized in Table 2. Overall, these findings included assessments of heterotopic ossification, radiolucencies, disc height, migration, subsidence, and loosening (Table 2). However, the reports lacked assessments of bone loss, and a range of methodologies was used by sponsors in radiographic assessments of cTDR, highlighting the need for standardization in this area. Similar findings have been reported for longer-term radiographic studies: a recent systematic review and meta-analysis aggregated all available 5 + year clinical outcomes for cTDR and reported that observations of bone loss/osteolysis were largely absent (or perhaps reported under other terminology or conditions) [32]. Only one reviewed study identified osteolysis, which was reported for six patients out of 715 [33]. Similarly, a recent analysis of shorter-term results found a low number of studies reporting osteolysis [34], and a review regarding cTDR radiological outcomes including HO lacked guidance on osteolysis/bone loss appearance [35]. While reports of radiolucencies were more common in the SSEDs and clinical trials, explanation of the assessment criteria used were often lacking. In our assessment, we considered progression of radiolucencies to be an additional and more telling indicator of the bone-implant interface. Thus, our study adds to the body of clinical findings by highlighting a bone loss metric that was perhaps poorly understood when these trials were designed and warrants continued research even today.
Using the proposed classification system, we observed reasonable agreement among experienced investigators. Previous researchers have employed classification systems for anterior bone loss around cTDRs [28, 29], rather than assessing the anterior, centralized, and posterior regions of the endplates as we proposed in the present study. In addition, previous investigators did not assess the repeatability or reproducibility of their classification systems for anterior bone loss, making it difficult to compare prior research with the present study. Chen and colleagues [29] evaluated radiographs of the Bryan disc for anterior bone loss, with a grade ranging from 0, with no bone loss, to 2 for “obvious bone regression.” They found that anterior bone loss with a Grade of 1 or 2 occurred in the inferior endplate of 54/121 patients (44.6%) from their series within the first 6–12 months after surgery [29]. Kaiser et al. [28] performed radiographic measurements of the relative distance of anterior bony coverage by the endplates of three different cTDR designs over time. The researchers assessed the anterior bone loss as minor (< 5%), moderate (5–10%), and severe (> 10%). Among the 156 cTDR evaluated, Kaiser [28] found anterior bone loss in 57.1% of cases evaluated. In our study, we found that binary radiographic assessments, such as the presence of absence of bone loss in a particular location, as well as subsidence, migration, and progressive core height loss, were found to exhibit the highest agreement among investigators. Lower agreement was found in our study among investigators when grading the severity of bone loss, indicating the lack of consensus as to what constitutes mild, moderate, or severe bone loss. For example, Kaiser [28] considered 10% of anterior bone loss to be severe, whereas the investigators in the present study considered loss of 1/3 of the endplate coverage to be severe. With regard to the accuracy of the proposed classification system, we expect that broad use of the tool by experts will help establish “gold standard” classifications which can be used to assess validity in future work. Our study confirms the utility of the HO classification system proposed by McAfee et al. [18] Because HO can occur in some regions of a cTDR that also are undergoing bone loss, we consider it important to include HO assessment in the characterization of bony changes using radiographs.
We would like to underscore several limitations for the reader. In the present study, we focused on developing a classification system for plain radiographs because of their ubiquity in clinical follow up of spine patients. However, plain radiographs can underestimate bone loss. Variations in imaging technique, such as tilting or obliquity of the cTDR with respect to the plane of radiographic study, greatly complicate the assessment of the bone-implant interface. Differences in radiographic exposure over time can also confound the interpretation of the bone-implant interface, if insufficient or inconsistent beam penetration of the bone occurs over time. Additionally, the presence of bony or radiographic abnormalities can also affect the interpretation of the radiographs. These limitations may help explain, in part, the lower agreement in the assessment of bone loss severity among investigators, and lower-quality radiographs may complicate use of the classification system in practice. In addition, plain radiographs have limitations in diagnosis of the underlying causes of the bone loss, and whether the mechanism in a particular patient is due to a septic or aseptic etiology [25]. Furthermore, it can be challenging to assess whether loosening is caused by failure to achieve initial stable fixation of the metallic endplates. Although the progression of radiolucencies can be useful in this regard, subtle bone-implant relative motion may also be appreciated by alternating flexion and extension views while the images are stabilized on the superior and/or inferior vertebral body. We did not consider such flexion–extension image assessment as part of the present study. We similarly did not consider AP view radiographs, which restricted our ability to clearly explore changes occurring lateral to the implants. Despite these limitations, due to the prevalence of radiographs in cTDR patient care, improving the consistency in terminology and classification of radiographic changes at the bone-implant interface is expected to improve communication among clinicians.
Conclusions
In summary, a standardized nomenclature for bony changes following cTDR will facilitate accurate and reproducible scientific communications regarding the clinical outcomes of this procedure. The novel system proposed demonstrated good concordance among experienced investigators in this field and represents a useful advancement for improving reporting in cTDR studies.
References
Ostrov PB, Reddy AK, Ryoo JS, Behbahani M, Mehta AI. Anterior cervical discectomy and fusion versus cervical disc arthroplasty: a comparison of national trends and outcomes. World Neurosurg. 2022;160:e96–110. https://doi.org/10.1016/j.wneu.2021.12.099.
Byvaltsev VA, Stepanov IA, Riew DK. Mid-term to long-term outcomes after total cervical disk arthroplasty compared with anterior diskectomy and fusion: a systematic review and meta-analysis of randomized controlled trials. Clin Spine Surg. 2020;33(5):192–200. https://doi.org/10.1097/BSD.0000000000000929.
Bydon M, Michalopoulos GD, Alvi MA, Goyal A, Abode-Iyamah K. Cervical total disc replacement: food and drug administration-approved devices. Neurosurg Clin N Am. 2021;32(4):425–35. https://doi.org/10.1016/j.nec.2021.05.003.
Phillips FM, Coric D, Sasso R, Lanman T, Lavelle W, Blumenthal S, Lauryssen C, Guyer R, Albert T, Zigler J, Cammisa F, Milam RA. Prospective, multicenter clinical trial comparing M6-C compressible six degrees of freedom cervical disc with anterior cervical discectomy and fusion for the treatment of single-level degenerative cervical radiculopathy: 2-year results of an FDA investigational device exemption study. Spine J. 2021;21(2):239–52. https://doi.org/10.1016/j.spinee.2020.10.014.
Phillips FM, Geisler FH, Gilder KM, Reah C, Howell KM, McAfee PC. Long-term outcomes of the US FDA IDE prospective, randomized controlled clinical trial comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion. Spine. 2015;40(10):674–83. https://doi.org/10.1097/BRS.0000000000000869.
Gornet MF, Burkus JK, Shaffrey ME, Schranck FW, Copay AG. Cervical disc arthroplasty: 10-year outcomes of the Prestige LP cervical disc at a single level. J Neurosurg Spine. 2019;31(3):317–25. https://doi.org/10.3171/2019.2.SPINE1956.
Lavelle WF, Riew KD, Levi AD, Florman JE. Ten-year outcomes of cervical disc replacement with the BRYAN cervical disc: results from a prospective, randomized, controlled clinical trial. Spine. 2019;44(9):601–8. https://doi.org/10.1097/BRS.0000000000002907.
Callanan G, Radcliff KE. Cervical total disc replacement: long-term outcomes. Neurosurg Clin N Am. 2021;32(4):461–72. https://doi.org/10.1016/j.nec.2021.05.007.
Kim K, Hoffman G, Bae H, Redmond A, Hisey M, Nunley P, Jackson R, Tahernia D, Araghi A. Ten-year outcomes of 1- and 2-level cervical disc arthroplasty from the Mobi-C investigational device exemption clinical trial. Neurosurgery. 2021;88(3):497–505. https://doi.org/10.1093/neuros/nyaa459.
Denaro V, Papalia R, Denaro L, Di Martino A, Maffulli N. Cervical spinal disc replacement. J Bone Jt Surg Br Vol. 2009;91(6):713–9.
Guyer RD, Albano JL, Ohnmeiss DD. Cervical total disc replacement: novel devices. Neurosurg Clin N Am. 2021;32(4):449–60. https://doi.org/10.1016/j.nec.2021.05.004.
Zavras AG, Sullivan TB, Singh K, Phillips FM, Colman MW. Failure in cervical total disc arthroplasty: single institution experience, systematic review of the literature, and proposal of the RUSH TDA failure classification system. Spine J. 2022;22(3):353–69. https://doi.org/10.1016/j.spinee.2021.08.006.
DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop. 1976;121:20–32.
Gruen TA, McNeice GM, Amstutz HC. “Modes of failure” of cemented stem-type femoral components: a radiographic analysis of loosening. Clin Orthop Relat Res. 1979;141:17–27.
Vanrusselt J, Vansevenant M, Vanderschueren G, Vanhoenacker F. Postoperative radiograph of the hip arthroplasty: what the radiologist should know. Insights Imaging. 2015;6(6):591–600. https://doi.org/10.1007/s13244-015-0438-5.
Shin JJ, Kim KR, Son DW, Shin DA, Yi S, Kim KN, Yoon DH, Ha Y. Radiological changes in adjacent and index levels after cervical disc arthroplasty. Yonsei Med J. 2022;63(1):72–81. https://doi.org/10.3349/ymj.2022.63.1.72.
Dowdell JE, Kim JS, Mikhail C, Overley SC, Levin JM, McAnany SJ, Mroz TE, Hecht AC. The rate of heterotopic ossification following cervical disc arthroplasty: a systematic review and comparison of data. Spine. 2020;45(18):E1197–202. https://doi.org/10.1097/BRS.0000000000003524.
McAfee PC, Cunningham BW, Devine J, Williams E, Yu-Yahiro J. Classification of heterotopic ossification (HO) in artificial disk replacement. J Spinal Disord Tech. 2003;16(4):384–9. https://doi.org/10.1097/00024720-200308000-00010.
Wahbeh JM, Park SH, Campbell P, Ebramzadeh E, Sangiorgio SN. The lexicon for periprosthetic bone loss versus osteolysis after cervical disc arthroplasty: a systematic review. Eur Spine J. 2022;31(4):830–42. https://doi.org/10.1007/s00586-021-07092-9.
Josse J, Valour F, Maali Y, Diot A, Batailler C, Ferry T, Laurent F. Interaction between staphylococcal biofilm and bone: How does the presence of biofilm promote prosthesis loosening? Front Microbiol. 2019;10:1602. https://doi.org/10.3389/fmicb.2019.01602.
Hodges NA, Sussman EM, Stegemann JP. Aseptic and septic prosthetic joint loosening: impact of biomaterial wear on immune cell function, inflammation, and infection. Biomaterials. 2021;278:121127. https://doi.org/10.1016/j.biomaterials.2021.121127.
Prendergast PJ, Huiskes R. The biomechanics of Wolff’s law: recent advances. Ir J Med Sci. 1995;164(2):152–4. https://doi.org/10.1007/BF02973285.
Albanese CV, Rendine M, De Palma F, Impagliazzo A, Falez F, Postacchini F, Villani C, Passariello R, Santori FS. Bone remodelling in THA: a comparative DXA scan study between conventional implants and a new stemless femoral component. A preliminary report. Hip Int. 2006;16(Suppl 3):9–15. https://doi.org/10.5301/hip.2009.4849.
Aspenberg P, van der Vis H. Fluid pressure may cause periprosthetic osteolysis. Particles are not the only thing. Acta Orthop Scand. 1998;69(1):1–4. https://doi.org/10.3109/17453679809002344.
Bauer TW, Schils J. The pathology of total joint arthroplasty. II. Mechanisms of implant failure. Skelet Radiol. 1999;28(9):483–97. https://doi.org/10.1007/s002560050552.
Price RL, Coric D, Ray WZ. Cervical total disc replacement: complications and complication avoidance. Neurosurg Clin N Am. 2021;32(4):473–81. https://doi.org/10.1016/j.nec.2021.05.006.
Scott-Young M, Rathbone E, Grierson L. Midterm osteolysis-induced aseptic failure of the M6-C cervical total disc replacement secondary to polyethylene wear debris. Eur Spine J. 2022;31(5):1273–82. https://doi.org/10.1007/s00586-021-07094-7.
Kieser DC, Cawley DT, Fujishiro T, Tavolaro C, Mazas S, Boissiere L, Obeid I, Pointillart V, Vital JM, Gille O. Anterior bone loss in cervical disc arthroplasty. Asian Spine J. 2019;13(1):13–21.
Chen TY, Chen WH, Tzeng CY, Huang CW, Yang CC, Chen HT, Chang CC, Lee CY, Tsou HK. Anterior bone loss after cervical Bryan disc arthroplasty: insight into the biomechanics following total disc replacement. Spine J. 2020;20(8):1211–8. https://doi.org/10.1016/j.spinee.2020.04.017.
Ulivi M, Orlandini LC, Meroni V, Lombardo MD, Peretti GM. Clinical performance, patient reported outcome, and radiological results of a short, tapered, porous, proximally coated cementless femoral stem: results up to seven years of follow-up. J Arthroplasty. 2018;33(4):1133–8.
Efron B, Tibshirani RJ. An introduction to the bootstap. New York: Chapman & Hall; 1993.
Wahbeh JM, Bogosian CJ, Kistler NM, Park S, Ebramzadeh E, Sangiorgio SN. Combining all available clinical outcomes on cervical disc arthroplasty: a systematic review and meta-analysis. J Orthop Orthop Surg. 2022.
Skeppholm M, Henriques T, Tullberg T. Higher reoperation rate following cervical disc replacement in a retrospective, long-term comparative study of 715 patients. Eur Spine J. 2017;26:2434–40.
Joaquim AF, Lee NJ, Lehman RA, Tumialán LM, Riew KD. Osteolysis after cervical disc arthroplasty. Eur Spine J. 2020;29:2723–33.
Kani KK, Chew FS. Cervical disc arthroplasty: review and update for radiologists. Semin Roentgenol. 2019;54(2):113–23. https://doi.org/10.1053/j.ro.2018.06.001.
Acknowledgements
The authors would like to thank Stuart Pratt, Erin Johnson, Ph.D., and Hannah Spece, Ph.D. for their helpful discussions and contributions to the manuscript.
Funding
Support for this research was received from Orthofix.
Author information
Authors and Affiliations
Contributions
All of the authors, working collectively in a research committee, jointly contributed to the conception of the study, interpretation of the radiographs, and analysis of the data. AK, FP, and TL contributed cases for review; SMK and AK wrote the main manuscript text; FP, TL, GA made substantive revisions of the work. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
Support for this research was received from a manufacturer of cervical total disc replacements. Relevant financial activities outside the submitted work: board membership, consultancy, grants, royalties, payment for lecture.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Fig. S1.
Examples of endplate rounding. Fig. S2. Examples of cystic erosion with diffuse margin adjacent to endplate. Fig. S3. Examples of cystic erosion with sclerotic margin adjacent to endplate. Fig. S4. Example of cystic erosion (red arrow) along with endplate rounding (yellow arrow).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Khachatryan, A., Phillips, F.M., Lanman, T.H. et al. Proposal for a classification system of radiographic bone changes after cervical disc replacement. J Orthop Surg Res 19, 218 (2024). https://doi.org/10.1186/s13018-024-04679-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-024-04679-y